
When Medicine Needed Spirits:
How Prohibition Constrained Pharmacy Compounding and changed the landscape of pharmacy forever

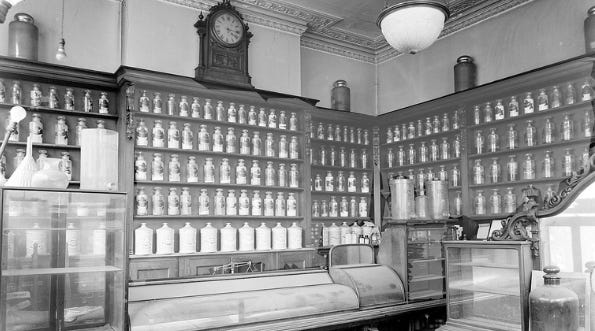
Herbal tinctures were well known to me through my early herbal trainings. What was not taught to me in pharmacy school was that tinctured medications were anchors in compounding in our pharmacies. In early 20th-century American pharmacy, alcohol wasn’t just a beverage it was infrastructure. Ethanol was a core solvent and preservative used to extract plant constituents, keep preparations microbially stable, and deliver medicines in palatable forms such as elixirs, aromatic spirits, and many cough and tonic formulas. When National Prohibition began in January 1920, pharmacies didn’t stop making medicines, but the legal and supply environment changed so sharply that it inhibited routine pharmaceutical work, pushed reformulation, and tangled legitimate practice with enforcement and suspicion.
Even before Prohibition, medical opinion about whiskey/brandy as therapeutics was shifting; for example, whiskey and brandy were removed from the list of scientifically approved medicines in the U.S. Pharmacopeia in 1916, reflecting growing skepticism about beverage spirits as “drugs.”
But that didn’t eliminate ethanol’s importance to pharmaceutics. Countless preparations relied on ethyl alcohol as the best practical solvent for resins, volatile oils, alkaloids, and botanical actives, and as a preservative in an era before today’s manufacturing, packaging, and refrigeration norms.
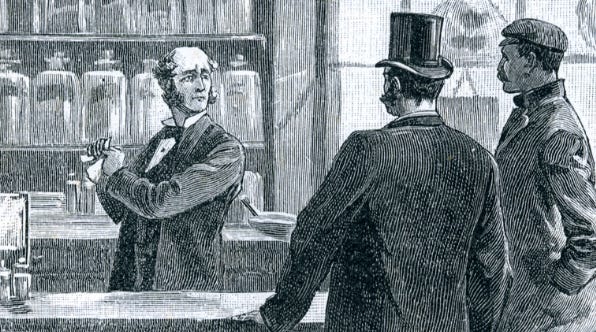
Prohibition arrived, the same substance that made a tincture possible was also the substance the federal government was trying to keep out of circulation. That meant pharmacies faced a new reality: alcohol wasn’t merely a reagent; it was a compliance risk.
To continue handling alcohol-containing products legally, pharmacies had to operate under a regulatory framework designed to prevent diversion. Contemporary museum archival summaries describe requirements such as applying for permits (renewed annually), posting security bonds, keeping logbooks of medicinal alcohol prescriptions filled, and maintaining monthly records of alcohol-containing products bought/sold.
Those burdens hit compounding pharmacies directly:
Administrative drag: time spent on compliance displaced time spent on formulation, patient counseling, and quality work.
Inventory friction: alcohol procurement and documentation became more complex, limiting the flexibility that compounding depends on.
Higher operating costs: bonds, recordkeeping systems, and the risk of penalties increased the “overhead” of making alcohol-based preparations.
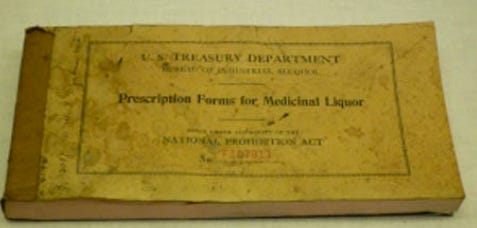
Prohibition law allowed alcohol for medicinal use under strict controls, but in practice it created a massive gray market routed through clinicians and pharmacies. The Smithsonian’s collections include official National Prohibition Act prescription forms for medicinal liquor as physical evidence of how formalized this channel became.
Multiple historical accounts describe limits such as a pint every ten days on government forms and “canceling” prescriptions after filling rules aimed at preventing refills and reuse.
Yet the scale of use was enormous: historical pharmacy sources estimate millions of alcohol prescriptions were written annually during the 1920s.


This mattered for medicine-making because it distorted incentives and scrutiny:
Pharmacies were treated (and sometimes behaved) like quasi-liquor outlets. That reputational shift made legitimate alcohol use for compounding more politically and legally sensitive.
Diversion fears encouraged tighter rules, which made legitimate practice harder (more audits, stricter paperwork, narrower allowances).
When alcohol becomes administratively “expensive,” practitioners adapt:
Reformulating away from ethanol (when possible) into glycerites, syrups, vinegars, oils, or lower-alcohol vehicles, often with stability or extraction tradeoffs.
Reducing on-hand stock to lower compliance exposure at the cost of creating a wait for their patients.
Avoiding certain formulations entirely because the recordkeeping and risk weren’t worth it, which would change the prescribing habits of our physicians and availability of medicines.
Even when Prohibition allowed specific medicinal alcohol channels, the system was not designed around pharmaceutical convenience, it was designed around preventing beverage use. The result was a practical inhibition: fewer preparations made the “easy” way, and some became economically or operationally unattractive.
As abuse of medicinal liquor channels became widely acknowledged, Congress and regulators moved toward additional control. By 1933, right before full repeal, Congress passed measures aimed at changing how medicinal liquor prescribing was handled by creating revised controls away from prescription blanks towards a stamp system.
Prohibition didn’t eliminate pharmacy compounding, but it made alcohol-based medicine-making harder, costlier, and riskier. Pharmacies had to navigate permits, bonds, meticulous logs, and heightened suspicion; they also operated in a landscape where “medicinal alcohol” became a heavily policed loophole rather than a straightforward pharmaceutical ingredient. The net effect was inhibition: less flexibility, more friction, and forced reformulation in the very years when many pharmacies still relied on alcohol as a primary tool of the trade.


While compliance costs and regulatory complexity weighed on smaller operators, larger chain pharmacies leveraged the medicinal alcohol loophole as a revenue driver. Walgreens, founded in 1901, was an early beneficiary:
In 1919 (just before Prohibition) it had around 20 stores.
By 1929, at the height of nationwide Prohibition, it had over 500 outlets across the U.S.
Because pharmacies could legally dispense alcohol with prescriptions and many customers sought that access, big chain drugstores became attractive destinations. The volume of prescriptions and foot traffic also boosted sales of other goods like sodas from in-store soda fountains, products that helped brands like Walgreens become household names.
Even beyond Walgreens, industry data from Drug Topics in 1928 showed thousands of chain drugstore units dominating the market and expanding across states like New York, Michigan, and Illinois.
There isn’t a detailed list of every drugstore that closed due to Prohibition, but multiple historical sources underscore a broader structural trend:
According to Drug Topics, the surge in chain drugstores in the late 1920s squeezed independents, as bigger networks could handle the paperwork and volume of medicinal alcohol business more efficiently and offer more general merchandise.
Independent pharmacies before the era numbered in the tens of thousands across the country; by mid-century, their proportion declined as chains gained scale and market share.
Histories of the profession note that the 1920s were a troubled decade for community pharmacy because the business model shifted away from traditional compounding toward retail dispensing and broader commercial products.
Even if Prohibition wasn’t the only cause of closures, it accentuated competitive pressures at a pivotal moment in the industry’s evolution. Many independents simply couldn’t match the operational capacity, marketing reach, and administrative infrastructure of emerging chains.
The 1920s and 1930s marked a turning point in how pharmacies operated:
Chain growth: By the late 1920s, chains like Liggett and Walgreens were counting hundreds of stores nationwide, pressuring independent drugstores to compete for customers and regulated prescription revenue.
Shift in role: The traditional role of pharmacists as compounders and personalized medication makers was already declining in favor of dispensing manufactured formulations, a trend accelerated by regulated alcohol sales and later industrial pharmaceutical production.
Long-term decline of independents: Over the ensuing century, independents continued to shrink as a share of the market. By the late 20th and early 21st centuries, independent pharmacies accounted for far fewer outlets as chains and big-box retailers dominated distribution.
While Prohibition’s medicinal alcohol loophole was an important economic lever in the 1920s, it worked alongside other forces that transformed pharmacy:
Regulatory change: Formalized education and licensure requirements began shifting the profession toward standardized practice and away from traditional compounding.
Industrial medicines: The rise of mass manufactured drugs diminished the relative role of compounding.
Retail evolution: Drugstores increasingly sold convenience goods, sodas, and other consumer products, blurring the line between pharmacy and general retail.
These forces combined with the peculiar economics of regulated alcohol prescriptions helped shift business power toward larger retail pharmacy chains and away from the small, traditional apothecary model. By the end of the Prohibition era, the foundation for the modern pharmacy retail landscape, a landscape dominated by large chains and fewer independent apothecaries was firmly in place and ready for Rockefeller.
Fascinating read! Thank you Allison. So that’s how it all evolved … I remember the older pharmacies of the early 60’s. The article took me on a journey back in time … even in the early 60’s there was definitely less product, apart from pharmaceutical products for purchase, but I also remember when it began to evolve into selling sodas and candy! I very much appreciate your research and sharing of these articles. Thank you!!